

Conservative treatment has no role in the management of scoliosis - or does it ?
© Postural Physiotherapy, Bondi Junction NSW, www.posturalphysiotherapy.com.au
Scoliosis is defined as a lateral deviation of the spine, however the true definition of
scoliosis is slightly wider. Scoliosis is a three dimensional deviation of the spine:
the involved vertebrae of the spine shift laterally (sideways), rotate backward on the
convex side (creating a rib or lumbar hump) and change their saggital (front to back)
position. The diagnosis of scoliosis is made when the angle between the most
tilted vertebrae (Cobb angle) involved in the curve is more than 10 degrees. There
can be many curve profiles in scoliosis and there is no known cure. Scoliosis can
often be progressive and affected by many factors; however the chance of progression
is increased relative to degree of the curve and earlier age of onset.
There are different types of scoliosis (commonly defined by age of onset) and the
most common is Adolescent Idiopathic Scoliosis (AIS). The remainder of this article
will primarily address AIS and provide some insight into the decision making process
around conservative management of AIS.
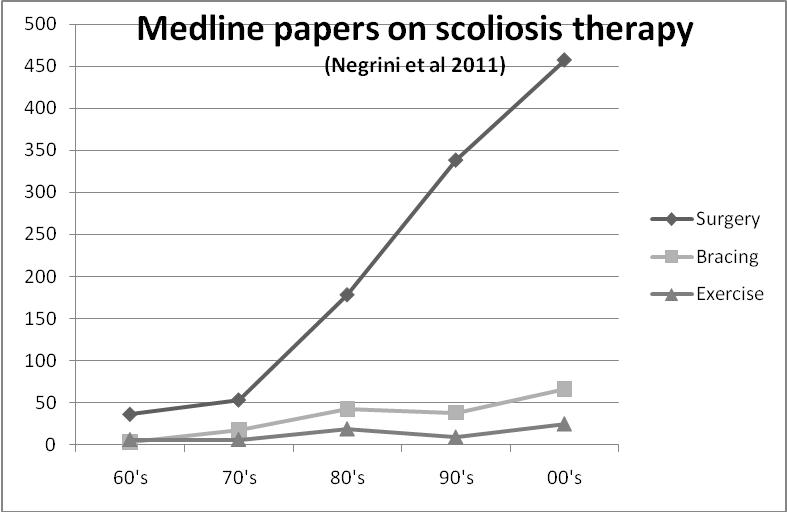
There is no doubt that there continues to be controversy with regard to the role of
conservative (non- surgical) management in scoliosis. There is a dearth of quality
information as seen in Figure 1.
Figure 1: (Negrini et al): A Medline search of all papers on scoliosis shows that
there is a massive difference in the amount of good quality research into conservative
management when compared to surgical management of scoliosis.
There are however many groups who are beginning to publish good research
into conservative management. Additionally, there are currently 2 international
groups conducting a randomised trial of Schroth treatment in scoliosis. One
group in Canada in a dual SRS, NIH funded trial under the auspices of Dr Eric
Parent and one group in England in a NHS funded trial under Warwick University.
Therefore, although there is no published evidence proving that Schroth works
there must be some benefit which has convinced these independent bodies to
contribute funds to these trials.
SOSORT (Society on Scoliosis Orthopaedic and Rehabilitation Treatment)
SOSORT (Society on Scoliosis Orthopaedic and Rehabilitation Treatment) is an
international group whose members include surgeons, doctors, physiotherapists,
chiropractors and bracing specialists who have a special interest in treating scoliosis.
SOSORT members believe in a team approach to the management of scoliosis
using all available techniques, including surgery, bracing and in some cases;
specific exercise therapy. SOSORT decision guidelines1 are assisted by the
following graph (Figure 2), which is based on Lonstein and Carlson's
progression estimation formula.
Progression factor = Cobb angle – (3 X Risser Sign) / Chronological age
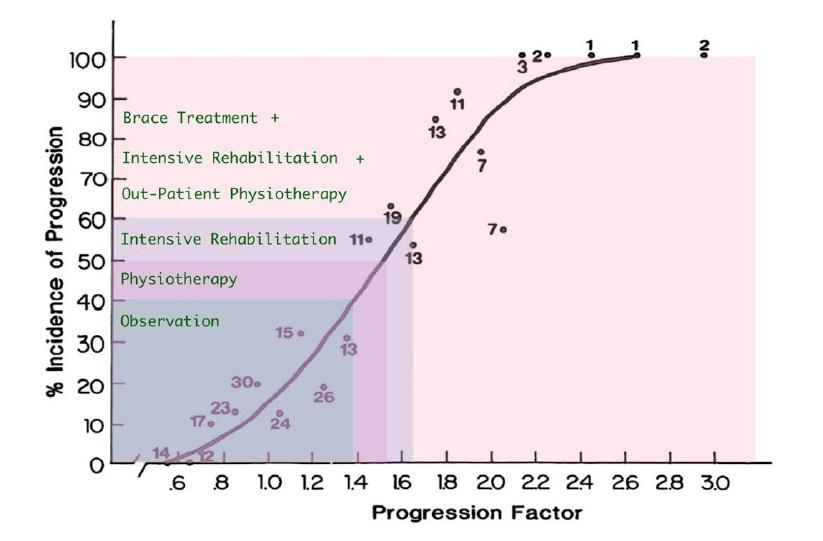
Figure 2: Progression risk above 40% is an indication for intervention. If
conservative management is unsuitable or fails then surgery is indicated.
The formula was originally based on curves 20-29 degrees so this needs
to be taken into account with larger curves.
For example, a 12 year-old girl with a 30 degree cobb angle and Risser 0 results in a
progression factor of 2.5 (30 degrees – (3 X 0) divided by 12. The risk of progression
is 90%. The treatment recommendation is bracing with exercises with close monitoring
and surgery if required.
Curves below 40% risk of progression are initially managed by observation alone
however curves at greater risk of progression require intervention. The intervention
can be specialised exercises, bracing or surgery. There are many type of braces
available but it is important to note that the person fitting the brace needs expert
knowledge of scoliosis and tracks the brace effectiveness with in-brace as well as
out-of brace x-rays. The patient will need to exercise to reinforce the brace action
and strengthen their musculature to ensure that there is no collapse upon brace
weaning. Furthermore the patient needs to be taught to internalise new body
image awareness and reflex curve correction. The curve correction is a
highly specialised specifically choreographed order of movements encompassing
all thee dimensions of the curve.
How does scoliosis occur?
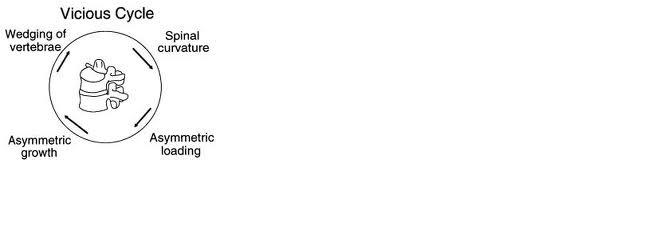
Stokes in 1996, 2000 and 2006 continued to expand on his resurrected ‘vicious cycle’
concept. The idea is that a triggering event to precipitate the assymetrical loading of the
spine will result in assymetrical growth of the vertebrae, wedging of the vertebrae and
hence an ever-increasing spinal curvature. Simplistically; a small curve can eventually
reach a threshold whereby gravity and mechanics alone can cause the curve to progress.
This is especially relevant during the growth phase.
Figure 3: The vicious cycle of scoliosis progression
Logic dictates that reduction in the assymetrical loading will reduce some of the inherent
load of this vicious cycle. Schroth therapy is one of the ways of restoring balance and symmetry
to the spine.
How does Schroth therapy work?
The asymmetry of the curve needs to, identified and deconstructed. The deconstruction of the
curve profile is analysed according to the principles of Katarina Schroth who was noted for
scoliosis treatment in 1925 founded her clinic in Germany in 1961. The method has been
refined over the years but the principles have remained unchanged.
Once the curve is analysed, the patient is taught a choreographed sequence of movements,
breathing action and muscle contraction to lead to greater symmetry of the body.
Summary
- Conservative management has a role in scoliosis treatment.
- Conservative management does not replace surgery.
- Bracing is effective in scoliosis treatment but needs to be applied, monitored and weaned correctly.
- Exercise therapy is highly specialised and needs to take into account the 3 dimensions of the curve.
- Saggital curve profile is an essential component of scoliosis and incorrect self correction can lead to detrimental loading of the curve.
- Scoliosis is best managed and treated by a team of specialist bracing, surgical and exercise practitioners.
References
1. http://www.sosort.mobi/pdf/OldSOSORTGuidelines.pdf
2. Biomechanical spinal growth modulation and progressive adolescent scoliosis – a test of the
'vicious cycle' pathogenetic hypothesis: Summary of an electronic focus group debate of the IBSE
Ian AF Stokes, R Geoffrey Burwell, and Peter H Dangerfield
Scoliosis 2006, 1:16doi:10.1186/1748-7161-1-16 http://www.biomedcentral.com/content/pdf/1748-7161-1-16.pdf
3. Self-Correction of posture: Assessemnt of the quality of the movement accomplished by non-instructed school children. Stolinski L & Kotwicki T. Proceedings of the Annual meeting of the SOSORT, Barcelona 2011.