

Scoliosis Blog
November Scoliosis Ramble
History is not changed by situations or corporations but by individuals and their reactions to situations, positions or events. Katarina Schroth was an individual who decided to address a situation and developed her method accordingly. The method has been refined by other individuals and these individuals adapt and progress the method.
When I first encountred the Schroth method through Tamar Neuhouse of SOSORTshe mentioned that I should get in touch with Lou Ann Rivett who is a South African physiotherapist who treats scoliosis and had initially spent time with Tamar learning Schroth. Lou Ann and I communicated occasionally but things changed drastically when one of Lou Ann's patients moved to Sydney and requested that I assist with her scoliosis treatment.
Lou Ann's patient has a significant double major curve (greater than 50 degree) and is in a RSC brace which is based on the principles of Schroth. However her patients exercise program deviates from classic Schroth and hence our increase in communication.
Lou Ann was kind enough to allow me to spend a few days with her this week observing and trying to comprehend her approach to scoliosis management. She has developed an approach of treating scoliosis that would be applicable to the African continent where patients do not have the ability to spend significant time learning classic Schroth method. Additionally, she has the benefit of working closely with an orthotist trained to fit the RSC brace, which unfortunately we do not have in Australia. However, Jeb McIvenney has advised me that we will soon have access to the Gomez rigid bracing system. I also saw a night bracing system called the Providence Night Bracing system for "progressive" curves between 15 and 25 degrees.
Lou Ann is writing up her PhD thesis on her work and hopefully be publishing her work as soon as her thesis is over.
 |
September October Scoliosis Blog
Although unintentional this blog is becoming a diary of work every 2 months.
Since school holidays finished, a few adults have been undergoing treatment. Adult curves are interesting in that in the majority of cases there is no major concern for impending surgery. Some of the adults have already had surgery and some are not in surgical range. Adults attend Schroth for different reasons; some come because of pain and some to prevent their curves progressing. There is a thought that curves over 30 degrees in an adult will progress 1 degree per year. I will try to find the source of that comment.
here is a comment from DS:
Hi Larry! I just thought I’d let you know how I’m going with my Schroth regime.
It took me a few days to get the ‘equipment’ ready … it seemed like an eternity but was really only two days. And my sewing skills … well, that’s another story. At least the wedge & cushion are holding together much to my surprise. 4 or 5 mornings a week I do the program of exercises ….. I am supposed to be doing 5 sets of 5 reps aren’t I ? I used to find sitting for any period of time uncomfortable, needing to prop myself up on the right side. But now I just need to sit straight and maintain the correct posture and I minimal trouble. And when standing (and sitting), I am continually correcting. So, Larry, a huge thank you for teaching me how to manage the curves and twists! I know I should come back for a ‘tune up’, but may need to leave it until after December. In the meantime, I will get some photo’s of my progress and email them FYI.
I also had the opportunity to work with a very special 7 year old girl from Victoria named E. I have often said that Schroth therapy is ideally implemented after the age of 10 in females but E's mother is an osteopath and we agreed that we would introduce her to some of the concepts of Schroth now, so that when she needs to work at the age of 10 she has already experienced the technique. During E's time in the clinic I met up with Jeb McIvenney who has recently returned to Sydney from the UK. Jeb, who is a chiropractor, travelled the world teaching the Spinecore bracing course and is therefore one of the world's expert Spincore brace fitters. It somehow worked out that E met up with Jeb and now she is progressing well in her new Spinecore brace. I will follow up on her progress with interest.
I continue to get queries about our Schroth protocol and treatment aims. It seems that there is no standard treatment protocol for Schroth therapy. Barcelona and Wisconsin both treat over a fortnight, Germany and the UK treat for a month. I treat over a 5 day week. My reasoning is simple; Medicare only rebates 5 sessions of physiotherapy per calendar year. So when I started off the treatment protocol I started off with 5 treatment sessions over 5 days. As the sessions are one on one we can get through a great deal of quality work within the sessions. The goal of the week is that by the end of the week the patient is able to perform 20-30 minutes of effective Schroth exercise and to understand how and why they are doing those particular exercises and corrections. Once they have completed the week, we meet up every for months for revision and then again for another week when able to.
August Scoliosis Ramble
August has almost departed and it has been a very busy month.
Last month I ended the blog with.. to be continued..and was hoping to write more over the month but never had the chance to do so. I recognise that the text version of the method appears very complex, but the theory behind the method is very logical and simple. However in practice, it is time consuming to learn correctly and to perfrom correctly.
Patients often wonder why we need to allocate so much time to learning the method but once going through the process understand why it is necessary.
Over the next few articles I will try to describe the method more clearly as well as provide scoliosis related info.
 |
I saw this case this month who presented with moderate to severe cervical pain. She is approx 40 years of age and was diagnosed and went through initial treatment in the UK. What was striking with her reported history is that she recalls being told by her specialists never to have children because of her scoliosis. Current thoughts are that women with scoliosis are able to bear children and I recommend that you discuss concerns with your treating specialist. |
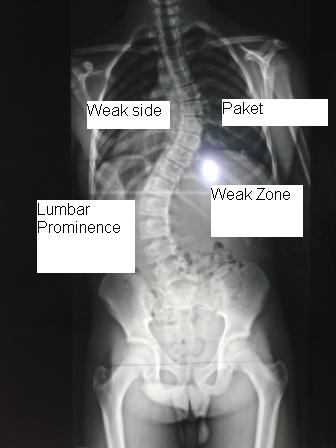 |
Alongside is a classic view of a scoliosis xray. I have inserted the Schroth terminology to define the particular areas of a scoliotic curve. This xray has the a right thoracic convex curve which is a very typical curve. The convex thoracic curve area on the body is termed the "Paket" and the concave thoracic side is called the "weak side". The convex lumbar curve to the left is called the lumbar prominence and its opposite concave side is called the weak zone. In the majority of curves the vertabrae of the convex areas will shift sidewards and rotate. This then causes a collapse of the concave side which is the reasoning for the term weak side. The rotated convex sides are seen as a rib hump or lumbar hump when bending over. |
 |
A view of the collapsed weak zone |
Last month I wrote about working with a special young man from Melbourne. Today I received the following email from his mother:
L had his Xray today and his cobb angle measures 29 degrees, compared to 38 on initial assessment with signs of some reduction in the rotation component of the curve (just looking at the spineous processes). We both feel very relieved that he has gained this amount of correction, and appreciated a surprised and positive response from Dr T(orthopaedic surgeon)!! Of course we are aware that once he is no longer wearing the brace he can regress, but he is certainly heading in the right direction.
Responses like these are always rewarding, and I hope that we can keep L heading in the right direction. I am further hopeful that if he can keep up with his exercises then we can build up sufficient strength and musculopostural (sorry- my own word) memory to maintain his corrections.
L returned for his follow up treatment today. He has been in his Boston brace for a few weeks and has been very committed with his exercises.
Below are his before and after x-rays.
 |
 |
| Image of Sept 2010 | Image of May 2010 |
July scoliosis ramble
YAY!!!! Its July.
Winter is here and we have had to ensure that the heating is on in the studio.
Quite a few patients who are now on school holidays have returned for their follow up reviews after commencing therapy between November and February. Some have done well, some have stayed the same but none appear to have regressed (curve progression). It does however appear that those who have done the best have been most compliant in their exercise program. It also appears that, over time, small unwanted compensations creep into the exercise positions and that these reviews are important to keep things on track.
Last week I had the pleasure of working with a very special young man from Melbourne who did very well during his sessions. He and his mother commented during his post session debrief that it would be beneficial to get some kind of idea about Schroth and the treatment regime we use before attending the first treatment session.
So.... here goes..
Schroth therapy aims to replace the existing scoliotic posture with a new posture that reduces and hopefully counteracts the scoliotic progressing forces. Lior Neuhause once stated that "if you can understand the curve, you can treat the curve". Therefore , the first part of the treatment protocol involves a comprehensive deconstruction of the components of the scoliotic curve and then a workshop period where the patient gets to "understand and internalise" their existing curve profile. This involves x-ray analysis, physical measurements and discussion.
Katarina Schroth called her technique 3 Dimensional treatment of scoliosis. We then apply the 3 dimensional correction protocol to the patients current existing curve profile. The Schroth technique is applied through a systematic series of postural corrections which are dependent on the curve profile. Over the course of the following week the systematic corrections are taught in a variety of starting positions. Once these postural corrections have been achieved then the patient is ready to commence specialised schorth breathing called Right Angled Breathing (RAB), which is an essential component of Schroth. The aim of the breathing is to expand the collapsed areas of the thorax and flank as well as to counter-rotate the chest wall and floating ribs in the abdomen.
Once we have achieved corrected posture, performing RAB we teach the patient activation exercises to strengthen the muscles that are required to maintian the new corrected posture.
to be continued
June Scoliosis Blog
It seems a bit repititous to say that "another month has gone by" but its true. We continue to stride along creating a healing environment to address postural and scoliotic issues.
I stayed up quite late a few nights ago to write this blog but somehow deleted the completed page before saving it. It was a good lesson... always save and backup.
When we were building the clinic, our builder; Blair, reported that the studio would make a great party venue for a ballet party. My daughter Gabrielle turned 7 last week and she requested a gymnastics party. Both Shana-Lee and myself are gymnastics coaches and a gymnastics party she had. It was wonderful seeing 21 little girls MOVING in the studio we created.
This month I received Martha Hawes updated book called Scoliosis and the human spine. I also received Nancy Schommer's book Stopping Scoliosis as well as David Wolpert's book Scoliosis surgery. The are all available through the American scoliosis assoc. here
Although not unexpected, it seems that the majority of the patients I am seeing have curve profiles around 40 degrees plus. They are all self referred or word of mouth referrals...Therefore.. these patients are probably in the group of probably or possibly heading towards surgery and as a last resort are willing to try physio because they have nothing else to lose. Reading the latter 2 books explains why there is such a reluctance to use physio as an option in idiopathic scoliosis treatment but reading the first book (Hawes) also provides fascinating reading of why it should be explored. I somehow don't seem to mind being classed as "you have nothing to lose by doing Schroth therapy" but I do have concerns when the argument claims "you have nothing to gain by doing schroth therapy".
Dr Rigo, on our intitial day of training, stressed that Schroth therapy is only one aspect of treatment and that we work in conjunction with all the other treatment providers. Martha Hawes is quite scathing in her thoughts regarding the "wait and see" approach to scoliotic curves. I don't agree with all her comments but there seems to be some logic in this. You might have nothing to lose by doing Schroth therapy and you might have something to gain (even if its only "muscular postural improvement and treatment of the parents psyche") but you definitly have nothing to gain by doing nothing.
We have been seeing quite a few adults over the last month. They differ from the adolescent patient in that their primary complaint is one of pain. It is important to note that the pain is NOT related to curve profile or whether they have had surgery or not. ie. a patient with a small curve might reports a great deal of pain whereas one with a large curve will not. Interestingly, idiopathic scoliosis in the adolescent is characterised by NO PAIN (although some authors disagree with this statement).
The treatment of the adult scoliotic is intersting as it might not be the curve that is causing their pain. They may, like 80 of the general population be suffering from "normal" musculoskeletal back pain. However they may not be... If my new patient reports in the history that they have, with limited success, already been treated with appropriate phyio, chiro or osteo.. etc. Then I have tended to commence treatment using Schroth based therapy. Results have been very positive.. quite a few of my patients are saying that when they do their exercises and adopt a better posture then it assists to resolve their pain. The goal is now to get them to maintain their corrected postures for great periods of the day.
May Scoliosis Ramble
Another month is flying by.
We have been in the clinic for almost a month. The reception desk arrived last week and the wall bars were installed today. It remains very exciting.
The studio is finally looking the way I envisaged. I had a new 14 year old patient today who was referred with acute knee pain and according to her mother "by the way, she has been told that she has scoliosis". The knee condition whilst significant is under control but the scoliosis which is VERY real needs to be investigated and managed. It is comforting to know that we now have a dedicated space to deal with these cases and that patients can feel reassured that we can provide excellent therapy in the correct environment.
We will be taking some photo's over the next week or two and I will upload them to the site.
At the end of the last months blog I wrote about the Canberra marathon. Thankfully as well as unfortunately its over. I managed to beat my previous marathon best (10 years ago) by almost an hour. Its amazing to recognise that during the massively busy period of setting up and moving clinics I was still able to train reasonably hard. I am now able to put more time into the clinic but miss the time on the road which I suspect my mind uses as "stress relief". Although I think its a good idea to stay out of political debate I think Tony Abbot's physical training regime is a GOOD THING. I wish I could complete an Ironman whilst being very busy and think he is an incredible athlete having only trained 10 hours per week.
This week is the SOSORT conference in Montreal. Unfortunately I cannot make it there as there is much to do in the clinic. Quite a few of the Schroth therapists from around the world will be there. I was lucky this week to have a chat to Lou-Anne Rivett who is a South African trained Schroth physio. We had a very interesting chat about her approach to scoliotic curves and we will continue to work together. She has been treating a patient for the last few years who has recently moved to Sydney. Lou-Anne was telling me that she was dreading "schlepping" on a plane from Johannesburg. I think that its much further from Sydney. This year I will look foward to the conference book and next year I hope to be at the conference in Barcelona.
If you do read this blog...... please send me an email with some of your scoliosis stories.
Goal for the month... get to meet some Scoliosis surgeons!!
March April Scoliosis Ramble
It is hard to believe how quickly time has flown this year.
This past week has been a momentous, or to use a word from Kill Bill (the movie)- Gargantuan step in the life of postural physiotherapy.
We have finally moved into our new space. I know.... its been very hush hush. I have been practicing out of a 15sqm room in a doctors surgery for the last 10 years and since returning from Wisconsin realised that to work in postural and scoliosis therapy I would need more space. Admittedly I have been looking for the right space for a few years but nothing ever worked out - till now.
The space started off as part of the garage of the Meriton serviced apartment block which was converted into office suites by Meriton. It was an empty shell when I first saw it, but with the help of Agi Sterling architect and Blair and Alex of Mammoth builders, we moved in on Monday. There are of course the standard teething problems such as the reception desk not being ready on time and the 10 station wall bars not being ready on time (hopefully both will be installed in the next week or two).
The initial aim is to continue the existing "practice" of postural physiotherapy. The thursday morning "osteoporosis" class had its first session in the space. It was great!! finally the class could, using the surround mirrors, see what I have been trying to tell them for years. We will be adding another osteoporosis class on Tuesdays.
Although it started off as the "osteoporosis class" its more of what I call an intuitive journey through movement. We will also be adding some classes aimed at total hip and total knee recepient patients as well as people with chronic shoulder pain.
Finally!!!! when we get up to speed, we will be adding specialist posture and scoliosis classes.
Speaking to Blair a few days ago.. when we were really rushing aound doing a milliion things at once he asked what I have been doing in my spare time.. well- training for the Canberra Marathon on the 2nd of May. Once that is out of the way I will be able to devote more time to the blog.
February Scoliosis Ramble
Another month has gone by and the learning curve continues.
Dr Rigo had a very insightful comment back in Wisconsin. When describing the concept of Schroth "work" to the patients attending the course he reminded them that it would take at least 30 min of daily effort and that the "work" had to be of a sufficient quality to affect the curve profile positively. He said that if the 30min felt like 2 hours then the intensity and concentration (and hence quality) was probably not as good as it should be; but if the 30 min felt like 5 min then the quality was probably good. This last month certianly has flown- hopefully because the quality and intensity of the work has been good.
Last month I commented on the reluctance of the SRS community to accept physiotherapy as a method to treat scoliosis. Their current accepted protocol accepts 2 methods of treatment. Surgery and Bracing. There are quite a few methods of bracing and previously in the blog I mentioned the RSC brace (Rigo style Cheneu brace) which is a rigid brace. Another kind of rigid brace is the Boston brace.
Over the last few months I have been treating quite a few patients who wear a non-rigid brace called the Spinecor brace http://www.spinecorporation.com/English/index.htm. This brace is very intersting in that it is (as stated) non rigid and also not readily accepted by the "recognised" spinal surgeons in Australia. There is a fair amount of literature around on the brace it appears that in some circumstances the rigid braces have been shown to be more effective than the non-rigid spinecore brace. However, spinecore maintain that the author's of the studies were not qualifed to fit the brace and hence their results were flawed.
Spinecore ran a brace fitting course last month in Melbourne. As I treat patients who use the brace and the fittiing of the brace is very important I decided to go along and do the course. Additionally, spinecore has a specific physiotherapy program which I wanted to do as well.
The course was very, very good and the trainer; an ex Aussie who is the internation R&D manager has a wealth of experience.
We reviewed both the adolescent bracing system and a new adult bracing system that Spinecore has recently released. The majority of the other attendants on the course were probably aiming to eventually get certified to prescribe the Spinecore brace however that was not my original intention in doing the course... at least now I have a better understanding on what the brace is trying to achieve.
January Scoliosis Ramble
Scoliosis work is continuing to move along steadily.
I was researching the SRS website (Scoliosis Research Society (predominately surgeons) who state that the only recommended treatment options for scoliosis is bracing and /or surgery. ALL other treatment modalities (including physical therapy) are termed alternative treatments and not endorsed as beneficial in the treatment of scoliosis. I have always strived for excellence in therapy and kept up to date with modern EFFECTIVE treatment techniques. It is distressing to realise that one of the "partners" in the scoliosis team is reluctant to acknowledge that Schroth might have a role in assisting the management of the curve profiles.
It is always daunting to commence a new treatment path, especially with such "high stakes" patients. I am verly lucky in that I have managed to harness the experience of Lior Neuhaus in Israel, Beth Janssen in Wisconsin and of course, Dr Rigo in Barcelona. We were very well trained in Wisconsin but there are always borderline cases that make contact hoping for advice regarding conservative management of their curves. I have been communicating with some "difficult" cases over the last few weeks and unfortunately I can see why some alternative care practitioners are causing the established medical community to hesitate when dealing with conservative management.
One case in particular involves a 12 year old girl with a 70 degree thoracic curve and a 35 degree lumbar curve. She is from interstate and has been visiting a "so-called" conservative management scoliosis expert overseas. This expert advised the family that the young girl would not need to wear her prescribed brace and that she should continue with her exercises using a special chair. I discussed the case with the group and we all agreed that unfortunately this is one case where conservative management is not indicated and is probably unethical to recommend. The danger is that this young girl could land up with a curve exceeding 100 degrees!
The SRS states that they cannot endorse alternative therapy because of a lack of peered reviewed medical journal articles supporting the different treatment approaches. There is probably a shortage of articles but they are being gradually added to the available literature. I think that inappropriate and dangerous recommendations on the part of so called "conservative management" specialists only adds to the reluctance of the mainstream medical partners (surgeons) to take us seriously.
I will hopefully over the next few weeks be making contact with some of the scoliosis experts and we'll have to see how things go.
December Scoliosis Ramble
Since my return from Wisconsin things have been very busy. I took a few sets of x rays with me to Wisconsin to review with Dr Rigo and have commenced treatment with these patients.
I would like to think that they are all doing very well but this sort of terminology is fraught with danger as “doing very well” encourages an expectation of improvement of Cobb angle where this is, in my mind, not the direct aim of the Schroth method.
It is important to recognise that the Scoliotic curve is a 3 Dimensional curve and that the Cobb angle measures only the lateral deviation of the spine. It does not indicate the rotation of the spine (which can be indicative of the magnitude of the rib hump), nor the saggital profile of the spine. This means that 2 people with the same Cobb angle can have totally different scoliotic curves and rib hump sizes. Therefore it is possible to encourage a better scoliotic curve without a measurable difference in Cobb angle.
The aim of the Schroth method is to teach the patient an alternate posture by gradually de constructing the existing scoliotic curve. It is possible and we have observed in our patients that the lateral translations can be centred and that the rib hump and lumbar prominences can be derotated and the collapsed areas of the thorax and lumbar region can be de-collapsed during the exercises. Whether or not this alternate “corrected” posture can be maintained in the long term depends on the patient. However, even intermittent unloading of the scoliotic torsion during the daily exercises is beneficial to the patient.
Each Schroth based scoliotic centre seems to have its own treatment protocol and we are currently refining ours. It seems that the best outcomes are achieved when we can see our patients more frequently and for longer periods in the initial stages. There is an initial steep learning curve for the patients to recognise what we are trying to achieve, to then internalise the process and then perform the movements and then perform them correctly.
I am tending to lean towards a treatment protocol we devised for an out of town visitor of 5 days of consecutive visits of between 2 and 3 hours. We were able to get through a great deal of work and this formed a very solid foundation to the program. We are seeing the same benefits when local patients attend treatment more regularly in the initial stages.
In order to perform Schroth exercise the patient will require a few props and devices. These items will be listed in the FAQ section.
Scoiosis Course complete
15 November 2009
After 12 intense days, very limited sleep, lots of ice-cream we wrote our final exams on Thursday.
We self marked half the exams and Dr Rigo reviewed the rest of the exams. I now like the rest of my colleagues doing the course qualified in Schroth based Scoliosis treatment from the Barcelona School Certification Course.

I have collected a few interesting articles on the conservative management of scoliosis using the Schroth method
|
|
|
|
|